
14.6 POJA-L6283+6271+6275+6274+6266+6270 Histochemical profile of Rhabdomyolysis III (human)
14.6 POJA-L6283+6271+6275+6274+6266+6270 Histochemical profile of Rhabdomyolysis III
14.6 POJA-L6283+6271+6275+6274+6266+6270 Histochemical profile of Rhabdomyolysis III (human)
(By courtesy of P. Poels MD, PhD , neurologist, (Dept. Neurology Radboud university medical center, Nijmegen, The Netherlands and H. ter Laak PhD Section Neuropathology, retired staff member Department of Pathology, Radboud university medical center, Nijmegen, The Netherlands)
Title: Histochemical profile of Rhabdomyolysis III (human)
Description:
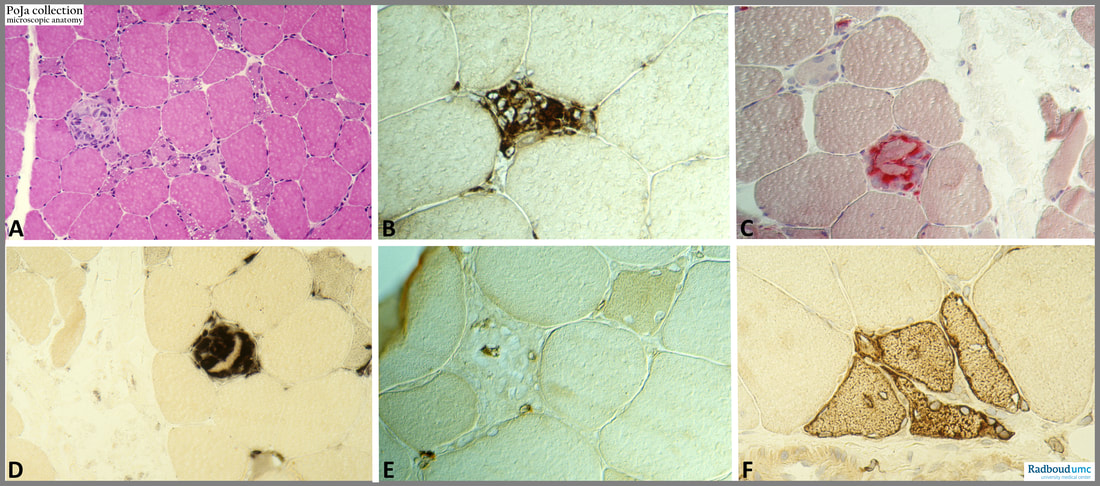
Muscle fibre necrosis is usually followed by myophagy and subsequent regeneration.
(A): Haematoxylin eosin stain. The image shows at the left a lighter stained fibre that is necrotic. However, there are still some normal stained components present. The myofibre itself is almost obscured by the presence of infiltrating cells and some nuclei of satellite cells. The latter will differentiate into regenerating myofibres.
The images (B – E) demonstrate myophagy of a myofibre.
(B): Immunoperoxidase stained with anti-macrophage antibodies.
(C) and (D) demonstrate the stained reaction products of two hydrolytic enzymes acid phosphatase (in red, C) and esterase (in black, D) respectively. The presence of these hydrolytic enzymes points to a strong phagocytic activity within the myofibres.
(E): A few CD3-postive T-cells are present too. These CD3-positive cells are involved in organising clearing processes of the degradation products.
(F): Locally satellite cells mature into regenerating myofibres distinctly stained transiently with Leu-19 (N-CAM epitope). (https://pubmed.ncbi.nlm.nih.gov/7685132/ )
Regenerating cells are smaller squeezed-like myofibres that sometimes contain central nuclei. Peripherally tiny vacuoles are present.
Background:
Rhabdomyolysis is caused by the breakdown and necrosis of muscle tissue and the release of intracellular content into the blood stream. There are multiple and diverse causes of rhabdomyolysis but central to the pathophysiology is the destruction of the sarcolemma membrane and release of intracellular components into the systemic circulation. The clinical presentation may vary, ranging from an asymptomatic increase in serum levels of enzymes released from damaged muscles to conditions such as volume depletion, metabolic and electrolyte abnormalities, and acute kidney injury. The diagnosis is confirmed when the serum creatine kinase (CK) level is > 1000 U/L or at least 5x the upper limit of normal. (https://pubmed.ncbi.nlm.nih.gov/32532456/ )
Keywords/Mesh: locomotor system, skeletal muscle, striated muscle, neuromuscular disease, myopathy, rhabdomyolysis, necrosis, degeneration, myophagy, pathology, POJA collection
Title: Histochemical profile of Rhabdomyolysis III (human)
Description:
Muscle fibre necrosis is usually followed by myophagy and subsequent regeneration.
(A): Haematoxylin eosin stain. The image shows at the left a lighter stained fibre that is necrotic. However, there are still some normal stained components present. The myofibre itself is almost obscured by the presence of infiltrating cells and some nuclei of satellite cells. The latter will differentiate into regenerating myofibres.
The images (B – E) demonstrate myophagy of a myofibre.
(B): Immunoperoxidase stained with anti-macrophage antibodies.
(C) and (D) demonstrate the stained reaction products of two hydrolytic enzymes acid phosphatase (in red, C) and esterase (in black, D) respectively. The presence of these hydrolytic enzymes points to a strong phagocytic activity within the myofibres.
(E): A few CD3-postive T-cells are present too. These CD3-positive cells are involved in organising clearing processes of the degradation products.
(F): Locally satellite cells mature into regenerating myofibres distinctly stained transiently with Leu-19 (N-CAM epitope). (https://pubmed.ncbi.nlm.nih.gov/7685132/ )
Regenerating cells are smaller squeezed-like myofibres that sometimes contain central nuclei. Peripherally tiny vacuoles are present.
Background:
Rhabdomyolysis is caused by the breakdown and necrosis of muscle tissue and the release of intracellular content into the blood stream. There are multiple and diverse causes of rhabdomyolysis but central to the pathophysiology is the destruction of the sarcolemma membrane and release of intracellular components into the systemic circulation. The clinical presentation may vary, ranging from an asymptomatic increase in serum levels of enzymes released from damaged muscles to conditions such as volume depletion, metabolic and electrolyte abnormalities, and acute kidney injury. The diagnosis is confirmed when the serum creatine kinase (CK) level is > 1000 U/L or at least 5x the upper limit of normal. (https://pubmed.ncbi.nlm.nih.gov/32532456/ )
Keywords/Mesh: locomotor system, skeletal muscle, striated muscle, neuromuscular disease, myopathy, rhabdomyolysis, necrosis, degeneration, myophagy, pathology, POJA collection