
|
POJA-L1800B+1801B+1802B+1804B
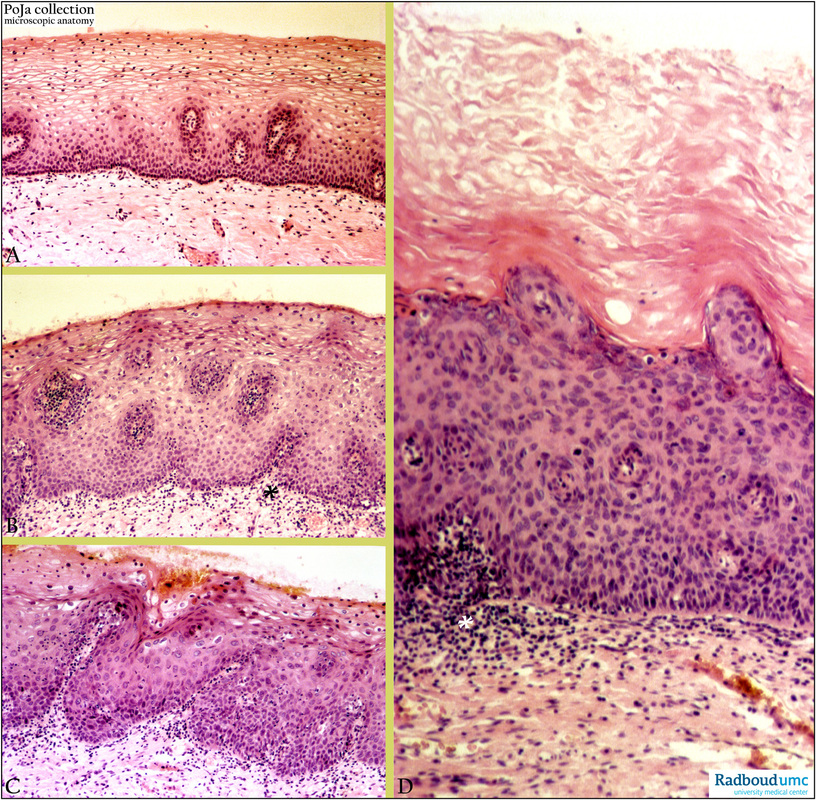
Title: Cervical intraepithelial neoplasm (CIN) (human, adult) Description: Stain: Hematoxylin-eosin. (A): Normal squamous epithelium of cervix. (B): CIN 1 (mild squamous dysplasia,) stroma with chronic inflammatory cells (*). (C): CIN 2-3 (moderate - severe squamous dysplasia), stroma with chronic inflammatory cells (*). (D): CIN 3 (severe squamous dysplasia - CIS with keratinisation), stroma with chronic inflammatory cells (*). (Partly by courtesy of G.P. Vooijs, MD PhD, former Head of the Department of Pathology, Radboud university medical center, Nijmegen, The Netherlands). |
Clinical background: Dysplasia or disordered growth is a reversible alteration that is marked by abnormal organisation, atypical cytology and increased rate of mitoses. This resulting abnormal cellularity implies altered polarity, differentiation and aberrant nuclear appearance in size and shape. The disordered development of immature basal cells of the cervical epithelium with an abnormal cell maturation usually starts at the squamocolumnar junction, often multifocally and involving the endocervical cleft. The severity of dysplasia is graded taking into account the nucleus/cytoplasm (N/C) ratio together with the loss of normal maturation:
Keywords/Mesh: female reproductive organs, cervix, CIS, CIN, HSIL, cervical intraepithelial neoplasia (CIN), carcinoma in situ (CIS), uterine cervical neoplasms,
- CIN 1 (mild dysplasia): epithelial disorganisation (compared to surrounding squamous epithelium), in lower 1/3 of epithelium undifferentiated high N/C ratio cells and in upper 2/3 presence of binucleated cells either enlarged/hyperchromatic or small, dense/hyperkeratotic, changes in cell arrangement with some loss of stratification of epithelium. Koilocytosis (perinuclear halo, nuclear pleiomorphism, hyperchromasia and often binucleation) might be present and is indicative for presence of HPV.
- CIN 2 (moderate dysplasia): in lower 2/3 of the squamous epithelium atypical basal cells and persistent abnormal differentiation towards intermediate and superficial cells with at least focal maturation, undifferentiated high N/C ratio cells, pleiomorphic and hyperchromatic nuclei, mitoses and loss of polarity in upper 1/3 of epithelium.
- CIN 3 (severe dysplasia as well as carcinoma in situ or CIS): atypical cells replace whole epithelium with loss of maturation, nuclear abnormalities more prominent in basal/parabasal cells, abnormal high N/C ratio cells with (often aberrant) mitoses through full thickness of epithelium, uniformly enlarged hyperchromatic nuclei crowded or irregularly spaced, pleomorphism and loss of polarity; surface parakeratotic cells with abnormal nuclei might be present and basement membrane is still found intact.
- Instead of the qualification CIS the synonymous term HSIL (high grade squamous intraepithelial lesion) is often used. High grade squamous intraepithelial lesion (HSIL) that corresponds to CIN 2 and CIN 3. Low grade squamous intraepithelial lesion (LSIL) that corresponds to CIN 1. Mild dysplasia (CIN 1) is usually caused by ‘low risk’ HPV (human papilloma virus) serotypes (a.o. 6, 11) and high-grade dysplasia (CIN 2-3) by ‘moderate risk’ (a.o. 31, 33, 35) and ‘high risk’ HPV serotypes (a.o. 16, 18)
Keywords/Mesh: female reproductive organs, cervix, CIS, CIN, HSIL, cervical intraepithelial neoplasia (CIN), carcinoma in situ (CIS), uterine cervical neoplasms,