
7.4 POJA-L4184+4185+4186. Ductal breast carcinoma in situ (DCIS) of cribriform type (human)
7.4 POJA-L4184+4185+4186
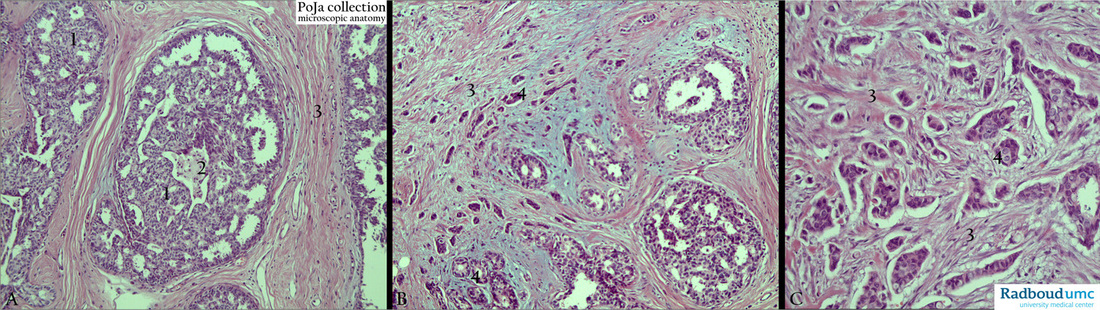
Title: Ductal breast carcinoma in situ (DCIS) of cribriform type (human)
Description: Stain: Hematoxylin-eosin.
(A): DCIS showing proliferation of relatively small and regular monophormic cells forming a ‘lacy’network of bridges and trabeculae of tumor cells (1). Partly necrotic luminal debris at (2) and at (3) periductal fibrous stroma.
(B): DCIS with rigid geometric epithelial bridges of monophormic tumor cells in coexistence with infiltrating ductal carcinoma, no-special type (NST). Invaded cords and tight clumps of tumor cells (4) in surrounding fibrous stroma (3).
(C): Ductal carcinoma-no special type composed of cords and sheets of small dense and large lighter cells (4) infiltrates in a disorganized way between the collagen bands (3).
(By courtesy of F. van de Molengraft MD PhD, Department of Pathology, Rijnstate Hospital, Arnhem, The Netherlands).
Background: Mamary carcinoma is divided into non-invasive (or in situ carcinoma) and invasive carcinomas. The former is categorized in comedo carcinoma in situ and non-comedo carcinoma in situ, both grouped as ductal carcinoma in situ (DCIS). The non-comedo carcinoma in situ is characterized by sculptures and well-defined formations of evenly placed hyperchromatic cells. These patterns are usually present as micropapillae of solid cells (papillary, micropapillary types) or as a network of cells separated by sharply defined circular, secondary spaces (cribriform type). The two patterns often coexist and coarse microcalcifications in necrotic luminal debris or fine clusters of calcifications in the interstices of epithelial proliferations form diagnostic features for mammographic detection. DCIS is usually confined to one quadrant of the breast and DCIS also often coexists with invasive tumors. Lobular carcinoma in situ (LCIS) is less common than DCIS, the epithelial proliferation of small, regular cells fills and distends the acini of one ore more lobules and frequently extends into terminal and subsegmental ducts. In contrast to DCIS, LCIS is often multifocal and bilateral involvement is reported (up to 30 % of the cases).
Keywords/Mesh: breast, mammary glands, breast neoplasms, ductal breast carcinoma, histology, POJA collection, cribriform,
Title: Ductal breast carcinoma in situ (DCIS) of cribriform type (human)
Description: Stain: Hematoxylin-eosin.
(A): DCIS showing proliferation of relatively small and regular monophormic cells forming a ‘lacy’network of bridges and trabeculae of tumor cells (1). Partly necrotic luminal debris at (2) and at (3) periductal fibrous stroma.
(B): DCIS with rigid geometric epithelial bridges of monophormic tumor cells in coexistence with infiltrating ductal carcinoma, no-special type (NST). Invaded cords and tight clumps of tumor cells (4) in surrounding fibrous stroma (3).
(C): Ductal carcinoma-no special type composed of cords and sheets of small dense and large lighter cells (4) infiltrates in a disorganized way between the collagen bands (3).
(By courtesy of F. van de Molengraft MD PhD, Department of Pathology, Rijnstate Hospital, Arnhem, The Netherlands).
Background: Mamary carcinoma is divided into non-invasive (or in situ carcinoma) and invasive carcinomas. The former is categorized in comedo carcinoma in situ and non-comedo carcinoma in situ, both grouped as ductal carcinoma in situ (DCIS). The non-comedo carcinoma in situ is characterized by sculptures and well-defined formations of evenly placed hyperchromatic cells. These patterns are usually present as micropapillae of solid cells (papillary, micropapillary types) or as a network of cells separated by sharply defined circular, secondary spaces (cribriform type). The two patterns often coexist and coarse microcalcifications in necrotic luminal debris or fine clusters of calcifications in the interstices of epithelial proliferations form diagnostic features for mammographic detection. DCIS is usually confined to one quadrant of the breast and DCIS also often coexists with invasive tumors. Lobular carcinoma in situ (LCIS) is less common than DCIS, the epithelial proliferation of small, regular cells fills and distends the acini of one ore more lobules and frequently extends into terminal and subsegmental ducts. In contrast to DCIS, LCIS is often multifocal and bilateral involvement is reported (up to 30 % of the cases).
Keywords/Mesh: breast, mammary glands, breast neoplasms, ductal breast carcinoma, histology, POJA collection, cribriform,