
14.6.1 POJA-L6194+6195 Inclusion body myositis (IBM): light microscopy (human)
14.6.1 POJA-L6194+6195 Inclusion body myositis (IBM): light microscopy
14.6.1 POJA-L6194+6195 Inclusion body myositis (IBM): light microscopy (human)
(Micrographs by courtesy of H. ter Laak PhD Section Neuropathology, retired staff member Department of Pathology, Radboud university medical center, Nijmegen, The Netherland)
Title: Inclusion body myositis (IBM): light microscopy (human)
Description:
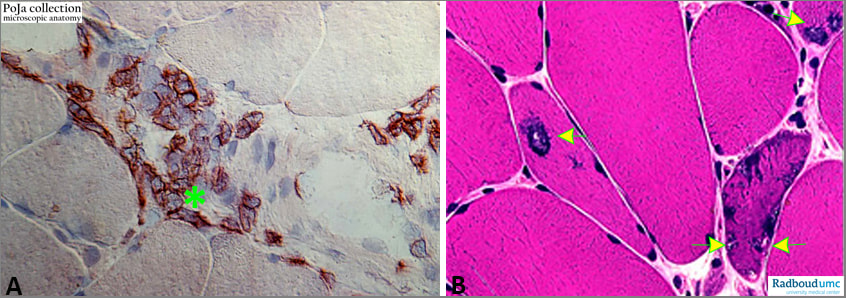
(A): Immunoperoxidase staining of infiltrate of CD8 positive T cells (*) in skeletal muscle.
(B): Rimmed vacuoles (arrows) in skeletal muscle fibre related to myositis.
Introduction: Inclusion body myositis (IBM) is one of the most common disabling inflammatory myopathies more commonly among males over 50. IBM is classified along with polymyositis, dermatomyositis as one of the idiopathic inflammatory myopathies. In contrast to the latter two disorders IBM is unresponsive to corticosteroid therapy. Symptoms of IBM are progressive weakness of the proximal muscles (wrists and fingers) and prominent weakness and wasting of the quadriceps muscle. The muscle involvement is often asymmetrical.
Aetiology: Genetic forms of IBM can be either dominant or recessive. The body’s immune system turns against its own muscles and damages muscle tissue in an autoimmune reaction. The identification of muscle-specific serum auto-antibodies and the increasing use of MRI in patients with IBM are important advances that may lead to earlier diagnosis and improved understanding of the disease. (Brady et al. Inclusion body myositis: clinical review and current practice Clin Pract 11, 623-637, 2014 ) .
Epidemiology: Inclusion-body myositis (IBM) primarily affects men. Patients progress to disability usually over a period of years. The older the age of onset is, the faster the loss of strength and mobility.
Pathophysiology: There are various degenerative changes in the muscle fibres with usually inflammatory cell infiltrates. Focally invasion of myofibres and linear distribution of inflammatory cells between the myofibres are observed. The inflammatory reaction is mainly composed of T-cells and macrophages with a predominance of CD8+ cytotoxic lymphocytes. Myofibres contain rimmed, granular vacuoles, filamentous inclusions and show upregulation of MHC-I expression. Muscle fibre sizes vary, apart from regenerating fibres hypertrophy occurs more commonly than in other immune myopathies.
See also:
Keywords/Mesh: locomotor system, skeletal muscle, striated muscle, neuromuscular disease, myositis, inclusion body myositis, IBM, rimmed vacuole, CD8 lymphocyte, T-lymphocyte, pathology, POJA collection
Title: Inclusion body myositis (IBM): light microscopy (human)
Description:
(A): Immunoperoxidase staining of infiltrate of CD8 positive T cells (*) in skeletal muscle.
(B): Rimmed vacuoles (arrows) in skeletal muscle fibre related to myositis.
Introduction: Inclusion body myositis (IBM) is one of the most common disabling inflammatory myopathies more commonly among males over 50. IBM is classified along with polymyositis, dermatomyositis as one of the idiopathic inflammatory myopathies. In contrast to the latter two disorders IBM is unresponsive to corticosteroid therapy. Symptoms of IBM are progressive weakness of the proximal muscles (wrists and fingers) and prominent weakness and wasting of the quadriceps muscle. The muscle involvement is often asymmetrical.
Aetiology: Genetic forms of IBM can be either dominant or recessive. The body’s immune system turns against its own muscles and damages muscle tissue in an autoimmune reaction. The identification of muscle-specific serum auto-antibodies and the increasing use of MRI in patients with IBM are important advances that may lead to earlier diagnosis and improved understanding of the disease. (Brady et al. Inclusion body myositis: clinical review and current practice Clin Pract 11, 623-637, 2014 ) .
Epidemiology: Inclusion-body myositis (IBM) primarily affects men. Patients progress to disability usually over a period of years. The older the age of onset is, the faster the loss of strength and mobility.
Pathophysiology: There are various degenerative changes in the muscle fibres with usually inflammatory cell infiltrates. Focally invasion of myofibres and linear distribution of inflammatory cells between the myofibres are observed. The inflammatory reaction is mainly composed of T-cells and macrophages with a predominance of CD8+ cytotoxic lymphocytes. Myofibres contain rimmed, granular vacuoles, filamentous inclusions and show upregulation of MHC-I expression. Muscle fibre sizes vary, apart from regenerating fibres hypertrophy occurs more commonly than in other immune myopathies.
See also:
- 14.6.1 POJA-L6092+6301+6340+6301B Inclusion body myositis (IBM): electron microscopy
- (https://emedicine.medscape.com/article/1172746-overview#a5)
Keywords/Mesh: locomotor system, skeletal muscle, striated muscle, neuromuscular disease, myositis, inclusion body myositis, IBM, rimmed vacuole, CD8 lymphocyte, T-lymphocyte, pathology, POJA collection