
14.6 POJA-L6305+6306 Myotubes and ATPase staining at pH 4.2 in striated muscle (human)
14.6 POJA-L6305+6306 Myotubes and ATPase 4.2 staining
14.6 POJA-L6305+6306 Myotubes and ATPase staining at pH 4.2 in striated muscle (human)
(By courtesy of H. ter Laak PhD Section Neuropathology, retired staff member Department of Pathology, Radboud university medical center, Nijmegen, The Netherlands)
Title: Myotubes and ATPase staining at pH 4.2 in striated muscle (human)
Description:
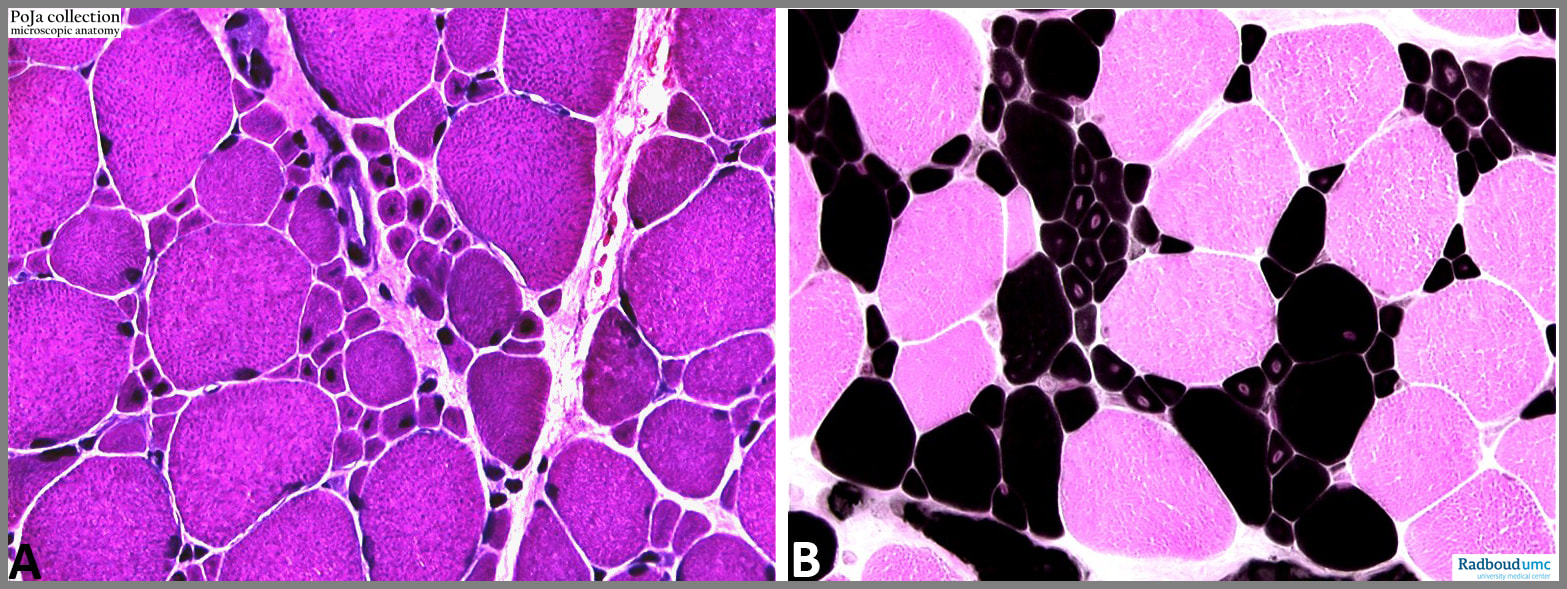
(A): Numerous small muscle fibres in the centre representing myotubes or myocytes with central nuclei (case myotubular myopathy), Haematoxylin-eosin stain.
(B): ATPase staining at pH 4.2. The dark brown smallest and larger myofibres are type I fibres known to contain slow myosin, the pink fibres are the type II ones (with fast myosin). In this case of myotubular myopathy as in many congenital myopathies type I fibres appear to be predominant and many fibres are small in diameter.
Background:
Primary myotubes presents as fused postmitotic myoblasts with large central nuclei and distinct nucleolus. Secondary myotubes develop by fusion of myoblasts along the surface of the primary myotubes. Thereafter the myotubes separate and each develops its own basement membrane. The early primary myotubes express one embryonic form of myosin heavy chain isoform. Subsequently under the influence of hormones, innervation the isoform differentiates into a foetal/neonatal form and the myotubes profile as either fast or slow myotubes.
Mostly primary myotubes profile as slow fibres expressing only slow myosin till the neonatal period. Secondary myotubes are hybrid fibres while they might express combinations of foetal/neonatal myosin fast and slow type (adapted from Dubowitz et al. 2013).
Keywords/Mesh: locomotor system, skeletal muscle, striated muscle, neuromuscular disease, myopathy, myotube, type I fibre, type II fibre, ATPase staining, myosin, pathology, POJA collection
Title: Myotubes and ATPase staining at pH 4.2 in striated muscle (human)
Description:
(A): Numerous small muscle fibres in the centre representing myotubes or myocytes with central nuclei (case myotubular myopathy), Haematoxylin-eosin stain.
(B): ATPase staining at pH 4.2. The dark brown smallest and larger myofibres are type I fibres known to contain slow myosin, the pink fibres are the type II ones (with fast myosin). In this case of myotubular myopathy as in many congenital myopathies type I fibres appear to be predominant and many fibres are small in diameter.
Background:
Primary myotubes presents as fused postmitotic myoblasts with large central nuclei and distinct nucleolus. Secondary myotubes develop by fusion of myoblasts along the surface of the primary myotubes. Thereafter the myotubes separate and each develops its own basement membrane. The early primary myotubes express one embryonic form of myosin heavy chain isoform. Subsequently under the influence of hormones, innervation the isoform differentiates into a foetal/neonatal form and the myotubes profile as either fast or slow myotubes.
Mostly primary myotubes profile as slow fibres expressing only slow myosin till the neonatal period. Secondary myotubes are hybrid fibres while they might express combinations of foetal/neonatal myosin fast and slow type (adapted from Dubowitz et al. 2013).
Keywords/Mesh: locomotor system, skeletal muscle, striated muscle, neuromuscular disease, myopathy, myotube, type I fibre, type II fibre, ATPase staining, myosin, pathology, POJA collection